MANAGEMENT OF FRONTAL SINUS FRACTURES – OUR EXPERIENCE
Marius Gabriel Dabija1,2, Sebastian Nechifor2, Vlad Andrei Dabija1,*, Cristian Dragoș Ștefănescu3,4, Răzvan Hainăroșie3,5, Cătălina Pietroșanu3,5, Corneliu Toader6, Andreea Rusescu3, Elena Oana Amza3, Octavian Dragoș Palade1,7
1“Grigore T.Popa” University of Medicine and Pharmacy, 2“Prof Dr. N. Oblu” Clinical Emergency Hospital, Iași,3“Carol Davila” University of Medicine and Pharmacy, 4“Gen. Dr. Aviator Victor Anastasiu” National Instituteof Aeronautical and Space Medicine, 5“Prof Dr Dorin Hociota” Institute of Phonoaudiology and Functional ENTSurgery, 6National Institute of Neurology and Neurovascular Diseases, Bucharest, 7“St. Spiridon” EmergencyUniversityHospital,Iași,Romania
Abstract: Frontal sinus fractures are one of the most devastating lesions that can occr after a high energy impact trauma. They are the expression of a severe cerebral trauma and in almost all the cases there are medical-legal implications. There is limited data, in Romania, regarding their management. Therefore, we attempt in this retrospective study to report our experience, following a 5-year period (2014-2019), in their treatment. Epidemiological and etiological data is exposed compared to the literature. We strongly think that a uniform treatment strategy of treatment, made by a multidisciplinary team, is mandatory.
Keywords: frontal sinus, fractures, trauma management.
1.INTRODUCTION
Compared to other anatomical areas of the cranial vault, the frontal sinus is exceptionally resistant upon infliction of external forces, making a fracture less likely to occur when following major trauma [1]. This fact is owed to the particular anatomy of the frontal bone, which evolved, in homo sapiens, primarily for containing the encephalon and secondarily for his protection. Sinus development is a result of anterosuperior pneumatization of the frontal recess into the frontal bone. Development begins late in intrauterine life or may start after birth (from one to twenty years), initially in the vertical segment. Pneumatization develops between ages 1-12 years.
This pneumatic cavity is bordered anteriorly and posteriorly by two bony tables. The structure of the anterior table is composed mainly by a thicker layer of cortical bone, than the posterior one, thus making it more resistant to external trauma. It can withstand between 800 to 2000 pounds of force before fracturing [2]. Consequently, fractures in this area, represent only 5-15% of all cranio-facial fractures [3]. The most common mechanism of injury is the application of an excessive and high velocity force, with a vector of direction perpendicular to the median sagital line. Very often the patients are victims of an aggression or an automobile accident and they frequently associate other injuries, thus making management difficult and raising significant medico-legal considerations.
The management of frontal sinus fracture patients is controversial and dependent on the type of fracture and the involvement of surrounding anatomical structures. The main concerns are aesthetics and the prevention of acute and delayed complications, which occur often and can be life-threatening or with significant loss of quality of life. The main complications are represented by cerebrospinal fluid leaking, meningitis, epidural abscess, brain abscesses, mucopyocele, osteomyelitis. Complications can appear years or decades after the initial traumatic episode and therefore the therapeutic algorithm is not straight forward, and it heavily relies on the sound judgement of the surgeon. In many cases, fast decision making based on scarce clinical and imagistic data, is required in the operating theatre. We believe that a standard and safe pathway in the management of this serious pathology is a must have in the “panoply” of a neurosurgeon.
The anatomic particularities that make these fractures prone to complications are caused by the structure of the posterior bone table. A relatively thin osseous barrier, between the colonized mucous membrane of the paranasal sinus cavities and the sterile meninges and brain, once compromised, can give rise to numerous infectious complications. Also once fractured, favored by its proximity to with the superior sagittal sinus, in rare circumstances, can cause the tearing of the venous sinus which will result in a very serious intracranial hemorrhage [4].
Surgical repair of comminuted frontal sinus fractures is not always easy to perform. The scattering of small bone fragments makes it difficult and time consuming to attempt a reconstruction with plates or wires and the result is often unstable, non-aesthetic and posing a high risk of postoperative complications. Specific bioinert materials, such as titanium meshes, aids us in the treatment of these types of severely comminuted fractures. We present our 5 year experience in frontal sinus fractures treatment and particularly, our experience of using titanium meshes in the surgical repair of the frontal bone defect.
2.MATERIAL AND METHODS
We present our experience in the treatment of frontal sinus fractures in a 5 year period and a review of the current management strategies offered by the literature.
Etiology of frontal sinus fractures
The most common etiology factor cited in the literature is represented by motor vehicle impacts. For an anterior table fracture to happen, because it’s tensile strength, it requires a great amount of energy applied directly. Motor vehicle accidents frequently can produce those types of forces. In a large series of patients treated for frontal sinus fractures (857 patients)Rodriguez et al. [5] reported motor vehicle collision as the cause in 42%, assaults in 14%, motorcycle collisions in 10% and pedestrian hit by a car while crossing the road in 8%. An interesting statistical fact of that study was the percentage of the passengers involved in car collisions which were unrestrained (not wearing seat-belt) – 60%.
In our statistical retrospective data on a five-year period (2014-2019) we hospitalized 665 patients with cranial fractures, and we diagnosed 78 patients with frontal sinuses fractures (11,72% of all cranial fractures). We noticed a difference regarding the etiology. In our series 22 patients (28.2%) were the victims of an human assault, 14 (17.94%) had motor vehicle accidents, 8 (10.25%) were the victims of a falling from heights, 7 (8.97%) of a falling from their own level, and 7 (8.97%)were victims of an animal assault. Most of the patients were male – 71(91%), and the average age in the series was 34.6years.
Clinical presentation and diagnosis
Clinical examination of these patients is impaired by facial hematomas, lacerations, edema, ecchymosis. Inspection and palpation of a depression of the frontal bone or other facial bone deformities is important, but mandatory is to establish the presence of the cerebrospinal fluid fistula, confirmed by the presence of CSF in an laceration or in the nose cavity (CSF rhinorrhea) which is a direct sign of posterior table breaching and tearing of the dura mater [6]. We believe that in the initial evaluation of a trauma patient a clinician identifying the presence of a CSF leak, even if it’s time consuming, is a key objective. The presence or absence of a CSF leak is a must have data needed for guiding the correct management protocol. Sometimes, in isolated cases of trauma patients presenting with clear rhinorrhea, quantifying glucose and beta-2 transfer in in the exudative fluid, is useful for distinguishing CSF from normal nasal discharge [6]. In our series 12 (15.38%) patients had a CSF leak at their initial presentation. Other common clinical findings in frontal bone fractures are represented by theability to feel or see bony fragments during laceration examination [7], supra-orbitary anesthesia and conjunctival ecchymosis. We consider that conventional plain skull radiographs even with specific sinus incidences are not useful for patients with suspected frontal sinus fracture. In our experience which align to the current standards reported in the literature, the preferable imaging used for the assessment of craniofacial traumatized patient is computed tomography (CT) [8]. It will provide, practically, almost all the information we need regarding bony elements of the face, the state of the nasofrontal ducts, and will confirm any intracranial associated lesions. Modern CT scanning allows multiplanar reconstructions, with detailed description of the type of fracture, structures involved, and therefore significantly influencing the management decision algorithm.
One of the most important structure to observe is the nasofrontal tract, it’s patency being of extreme importance in preoperative planning. Following a sound examination of scans, it is imperative to appreciate the type of fracture, the discontinuity of the sinus floor, the presence of CSF in the sinus, and note the degree of the displacement of the anterior and posterior table. Lastly, we must try not to overlook the intracranial and cervical spine lesions, which are associated frequently.
Classification of frontal sinus fractures
There were many classifications proposed for the frontal sinus fractures. However, the most accepted one, with the agreement among numerous authors (Luce, 1987; Wolfe and Johnson, 1988; Stanley, 1989;
Rohrich and Mickel, 1995; Gonty et al., 1999) [9-13] divides the fractures in:
-Anterior table fractures;
-Posterior table fractures;
-Anterior and posterior tables fractures;
-“Through and through” fractures (skin to anterior cranial fossa);
-Fractures involving the nasofrontal duct.
In our series we had 42 (53.84%) isolated fractures of the anterior table, 2 cases (2.56%) of isolated posterior table fractures and 34 (43.58%) with combined fractures of anterior and posterior tables.
In their large series, Rodriguez et al. [5] reported 38.3% anterior table fractures, 6.9% isolated posterior table fractures and 54.9% combined anterior and posterior tables fractures.
The problem of nasofrontal duct injuries is that they are not easily identified in head CT scans, and are often missed by the radiologist. This fact leads to under-reporting. In our database only 4 patients, had a fracture of this structure, mentioned in the initial radiology report, but, when we reanalyzed all the cases, we appreciated that the involvement of the nasofrontal duct was present in 51 cases (65.38%). A very important finding, as it influences the management, surveillance and outcome of sinus fractures.
Associated lesions and complications
Frontal sinus fractures, being the result of the exertion of high energy, makes the presence of cerebral associated lesions common, rather than an unusual finding. In our series, in 30 (38.46%) patients we diagnosed cerebral lesions: focal cerebral hematomas and contusions in 7 cases (8.97%), epidural hematomas in 10 cases (12.82%), subdural hematomas in 7cases (8.97%), subarachnoid hemorrhage in 6 cases (7.69%), pneumoencephalus in 14 cases (17.94%). Six patients were admitted in a coma state (GCS ≤ 8).
The complications in our series included: CSF fistulas in 12 patients (15.38%), meningitis in 2 patients (2.56%), diplopia in 3 patients (3.84%), frontal osteomyelitis in 1 case (1.28%). Other possible complications, not encountered in our series, include: frontal sinusitis, intracerebral abscess, empyema, cavernous sinus thrombosis, persistent CSF fistulas, limitation ofextraocular motions, mucocele/mucopyocele, frontal contour defects.
Treatment
Management of frontal sinus fractures, as previously stated, is controversial. There are, however, several principles of which the medical team must have strictly adherence, in order to successfully treat these patients:
-Prevention of early or delayed complications;
-Restoration of normal sinus function when is possible;
-Restoration of normal frontal bone shape and contour.
In the literature, treatment options described include observation, various types of reconstruction of the sinus walls, osteoneogenesis, ablation/exenteration, cranialization [3, 14-16].
In cases with anterior wall involvement, the primary purpose is often the cosmetic aspect. Fractures of the anterior wall may be without displacement or they can have various degrees of it. Most often, undisplaced fractures do not require surgical treatment, the only management consists in suturing skin defects and active surveillance to prevent potential complications. The same conservative treatment is recommended for the fractures with little displacement (1-2 mm).
If there is severe displacement of the bony fragments (2-6 mm) or significant comminution a surgical reduction maybe necessary, and most of the authors recommend correction with various types of fixations, in order to correct facial deformities and to prevent late complications as mucocele (Figs. 1, 2).
However, the risk of mucocele formation in isolated frontal sinus fractures is low, so, in our series we treated 9 patients with no reconstruction of the anterior wall, even comminuted, but, for cosmetic reasons, we performed cranioplasty with titanium mesh and left all the displaced fragments in place, with good results (Fig. 3).
The cosmetic result was excellent, and we encountered no infectious complications. All the patients had 5 days of antibiotic protection.
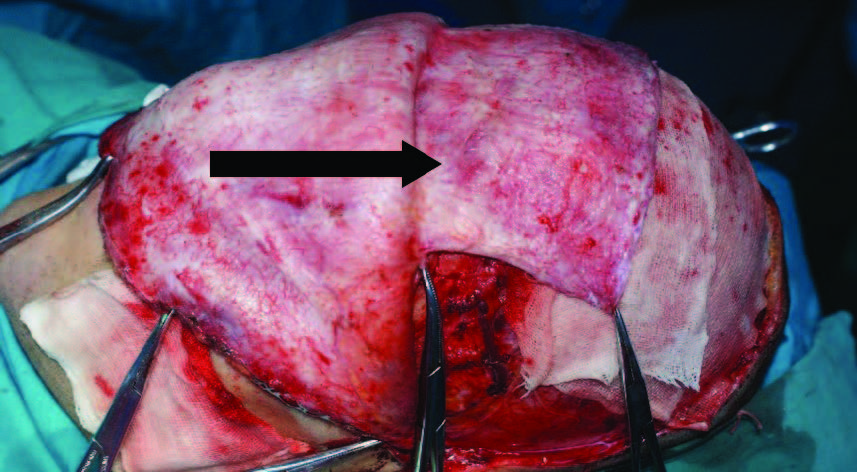
Figure 1. Exposure of epicranial flap after harvesting it.
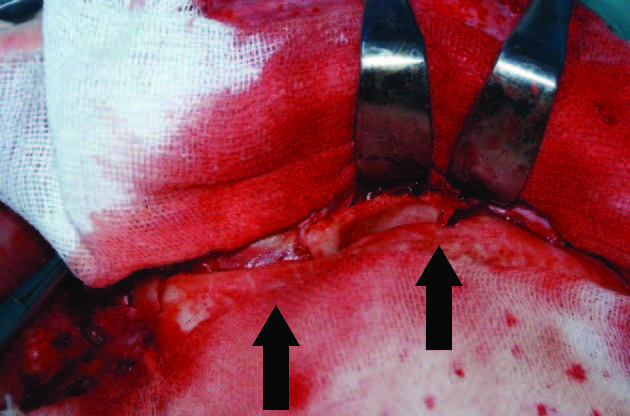
Figure 2. Exposure of anterior frontal wall fracture sites.
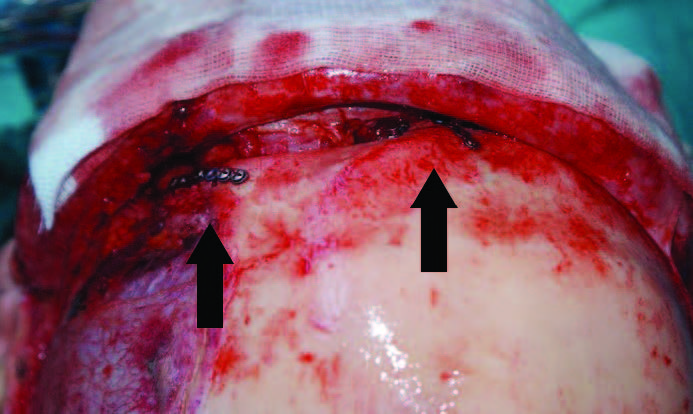
Figure 3. Reduction of the fracture using titanium plates.
Another possible issue is the involvement of the nasofrontal duct; various authors report an incidence of 25-50% [6, 15], especially when there is an association with orbital-ethmoidal fractures.
It is quite rare to have an isolated sinus of the posterior wall, most often there is a complex fracture involving also the anterior wall, ethmoid cells, nasofrontal duct, cribriform lamina. In a classic study, Nahum et al. [2] estimated the forces needed to fracture the posterior table, vary between 362 and 997 kg per square m2. In as many as a third of cases, a dural tearing [3] accompanies the fracture, creating a communication between the intracranial space and the nasal mucosa which increases the risk of meningitis. We experienced 12 cases of CSF leak and in only 2 cases we used a surgical approach to close the fistula; all the other patients had conservative treatment, in 7 cases a lumbar drainage was necessary. The goal of the surgery, used in patients carefully selected in which the CSF leak persisted more than 10-14 days despite all conservative measures, was the restauration of dural integrity and protection of the intracranial space by cranialization of the sinus and obliteration of the nasofrontal duct.
Obliteration of the frontal sinus consists in complete removal of the sinus mucosa, cauterisation of the walls, obliteration of the nasofrontal duct and filling the aeric space with various materials. There are autologous and alloplasticmaterials which can be used. Autologous materials may be fat, muscle, bone [5] and alloplastic bio-inert materials such as hydroxyapatite cement, methyl methacrylate, calcium phosphate bone cement, oxidized regenerated cellulose, bioactiveglass [7,17-18]. In our series, when the cranialization/ obliteration of the sinus was necessary, we used autografted bone fragments for filling the nasofrontal duct, after which we sealed it firmly with fat and fibrin glue and obliterated the rest of the sinus with autologous fat graft. The floor of the anterior cranial fossa is covered with a pedicled pericranial flap or lyophilizeddura.
3.DISCUSSION
Frontal sinus fractures raise important issues from the perspective of medical-legal activity. They are usually a consequence of an aggression or a vehicle accident, as in our series, where most of the patients (28.2%) were the victims of a human assault. The patients are relatively young (34.6 years in our series) but other authors reported even younger series between 21-30 years [19-20].
Isolated fractures of the anterior wall are the most frequent ones (53.84%) but there are studies which reported even a larger incidence of this type of fracture [20-21]. Frequently associated with esthetic issues, they can severely lower the quality of life. Thus, the repair of the frontal bone shape is in most of the cases, imperative, even when complex associated bony and skin lesions exists. In difficult to treat cases, from the aesthetic point of view, a multidisciplinary approach is recommended, preferably from a team formed by a plastic surgeon, a neurosurgeon, a ophthalmologist and a ENT surgeon [22].
Posterior table involvement, it is the result, in the majority of cases, of a high energy force of impact. An important medical-legal consideration, because, those forces occur especially in blunt weapon assault or shootings, and lesions can be used to quantify the severity of the aggression. Also due to the frequent association of cerebral lesions and local complications (CSF leak, meningitis, abscesses, mucoceles) that have to be prevented or treated implying a longer hospitalization, high treatment costs, and a longer convalescence. In our series the involvement of the anterior and posterior wall was 43.58% and the global rate of associated cerebral lesions was 38.46%. The prevalence is similar to that reported in literature statistical data [9,14,21].
We believe the future of treatment relies on the formulation of a standard management protocol, rooted in evidence-based medicine, being it conservatively or surgical, of frontal sinus fractures. Significant steps, on this pathway are made by the CMF branch of AO Foundation. S Fusetti et al., recently uploaded a digital library with summarized management guidelines, which can be accessed freely and readily by a surgeon in need [23]. Therefore greatly aiding in clinical decision making and subsequently improving the outcome of treatment [24].
In conclusion, sinus frontal fractures are rare, in comparison to other fractures of the cranial vault, are resultant of high energy of high impact trauma and raise significant socioeconomic and medico legal considerations. Frequently, these fractures are associated with intracranian injuries and crippling complications. There isn’t a single general strategy of management, so developing one based on systematic review and meta-analysis of the literature is mandatory.
Conflict of interest
The authors declare that they have no conflict of interest.
4.References
- Chen TM, Wang HJ, Chen SL, Lin FH. Reconstruction of post- traumatic frontal-bone depression using hydroxyapatite cement. AnnPlastSurg. 2004; 52:303-308.
- Nahum AM. The biomechanics of maxillofacial trauma. Clin Plast Surg. 1975; 2:59-64.
- Gerbino G, Roccia F, Benech A, Caldarelli C. Analysis of 158 frontal sinus fractures: current surgical management and complications. J CraniomaxillofacSurg 2000; 28(3):133–139.
- Donald PJ. Frontal sinus fractures in otolaryngology, head and neck surgery. Cummings. ed. St. Louis: CV Mosby Co. 1986: 901.
- Rodriguez ED, Stanwix MG, Nam AJ, St Hilaire H, Simmons OP, Christy MR, Grant MP, Manson PN. Twenty-six-year experience treating frontal sinusfractures: A novel algorithm based on anatomical fracture pattern and failure of conventional techniques. Plast Reconstr Surg. 2008; 122:1850-1866.
- Tiwari P, Higuera S, Thornton J, Hollier LH. The management of frontal sinus fractures. J Oral Maxillofac Surg. 2005; 63:1354-1360.
- Rohrich RJ, Hollier L. The role of the nasofrontal duct in frontal sinus fracture management. J Craniomaxillofac Trauma. 1996; 2:31-40.
- Stanwix MG, Nam AJ, Manson PN, Mirvis S, Rodriguez ED. Critical computed tomographic diagnostic criteria for frontal sinus fractures. J OralMaxillofac Surg. 2010; 68:2714-2722.
- Olson EM, Wright DL, Hoff man HT, Hoyt DB, Tien RD. Frontal sinus fractures: Evaluation of CT scans in 132 patients. AJNR Am J Neuroradiol.1992; 13:897-902.
- Luce EA. Frontal sinus fractures: Guidelines to management. Plast Reconstr Surg. 1987; 80:500- 508.
- Wolfe SA, Johnson P. Frontal sinus injuries: primary care and management of late complications. Plast Reconstr Surg. 1988; 82: 781-789.
- Rohrich RJ, Mickel TJ. Frontal sinus obliteration: in search of the ideal autogenous material. Plast Reconstr Surg. 1995; 95:580- 585.
- Gonty AA, Marciani RD, Adornato DC. Management of frontal sinus fractures: a review of 33 cases. J Oral Maxillofac Surg. 1999; 57:372- 379.
- Strong EB, Pahlavan N, Saito D. Frontal sinus fractures: A 28- year retrospective review. Otolaryngol Otolaryngol Head Neck Surg. 2006; 135:774-779.
- Bell RB, Dierks EJ, Brar P, Potter JK, Potter BE. A protocol for the management of frontal sinus fractures with emphasising sinus preservation. J OralMaxillofac Surg. 2007; 65:825- 839.
- Gossman DG, Archer SM, Arosarena O. Management of frontal sinus fractures: A review of 96 cases. Laryngoscope. 2006; 116:1357- 1362.
- Fattahi T, Johnson C, Steinberg B. Comparison of 2 preferred methods used for frontal sinus obliteration. J Oral Maxillofac Surg. 2005; 63:487-491.
- Kang GC, Sng KW, Tay AG. Modified technique for frontal sinus obliteration using calvarial bone and Tisseel glue. J Craniofac Surg. 2009; 20:528-531.
- Bell RB. Management of frontal sinus fractures. Oral Maxillofac Surg Clin North Am. Philadelphia. 2009; 21(2): 227– 242.
- Marzola, C. Fundamentos de Cirurgia e Traumatologia Buco Maxilo Facial. São Paulo: Ed. Big Forms. 2008; 6.
- Gerbino G, Roccia F, Benech A, Caldarelli C. Analysis of 158 frontal sinus fractures: current surgical management and complications. J Craniomaxillofac Surg. 2000;28(3):133-139.
- Ardeleanu V, Andronache LF, Gherghiceanu F, Paunica S, Balalau C. Treatment of lipomas and diffuse lipomatosis with NDYAG 1064 NM laser and their impact on the quality of life. Journal of Mind and Medical Sciences.2020; 7 (1): 16-22.
- Fusetti S, Hammer S, Kellman R, Matula C, Strong EB, Di Ieva A. Skull base & Cranial vault. AO Surgery Reference. https://www2. aofoundation.org/wps/portal/surgery?showPage=diagnosis&bone=CMF&segment=Cranium
- Stoian AP, Hainarosie R, Pietrosanu C, Rusescu A, Andronache LF. Modern concepts in non-surgical esthetics; a review. Journal of Mind and MedicalSciences. 2019; 6(2):190-195.